
The Use of Aspirin for Primary Prevention of Cardiovascular Disease: Review of Literature and Sample Evidence of Common Practice in Ireland
John Travers UCD School of Medicine and Medical Science, University College Dublin, Belfield, Dublin 4, Ireland
Dr. Helen Gallagher PhD, Senior Lecturer, School of Medicine and Medical Science, University College Dublin
ABSTRACT
The use of aspirin and broader anti-platelet therapy is well established for secondary prevention of cardiovascular (CV) events such as myocardial infarction, stroke or transient ischaemic attacks. However, there
is significant and growing evidence in the literature to conclude that the net benefits from taking aspirin for primary prevention (an unlicensed indication) are minimal and are counter balanced by harms such as gastrointestinal and extra- cranial bleeding.
Audits of GP practices suggest that prescription of aspirin for primary prevention is in fact common, despite the risks. Almost a fifth of patients taking aspirin in two practices in Dublin and Cork use the drug for primary prevention.
The risks and potentially fatal complications of bleeding should
be carefully considered and discussed with patients when prescribing aspirin
for secondary prevention of CV events and, on the basis of the most recent evidence, aspirin should not be routinely prescribed for primary prevention. A broader preventative approach such as addressing modifiable risk factors with patients at planned health checks can instead yield better overall outcomes. Guidelines on the use of aspirin in prevention of CV events should be updated to reflect the bleeding risks outlined in recent research.
Article
INTRODUCTION
Aspirin and its precursors have played a role in healthcare for millennia. It is said that Hippocrates offered pregnant women willow leaves in order to ease labour pains c400BC. The active ingredient of this traditional analgesic, salicylic acid, was first extracted from willow in the 19th century. Aspirin was synthesised by adding an acetyl group to salicylic acid to make it more tolerable for taking orally. Although one of the earliest drugs developed, aspirin is today one of the most commonly taken. Its use has expanded from pain relief to helping in the management of conditions such as cardiovascular disease (CVD), colon cancer and dementia.
Aspirin irreversibly inhibits cyclooxygenase (COX) enzymes that produce the prostanoid mediators of inflammation, resulting in anti-inflammatory, analgesic and antipyretic effects. COX inhibition also blocks aggregation of platelets. This reduces the risk of myocardial infarction (MI) or stroke due to thrombus formation following atherosclerotic plaque rupture.
The mechanism by which platelet aggregation is blocked begins with COX enzyme acetylation. There is a consequent reduction of thromboxane A2 (TXA2) synthesis in platelets and prostaglandin I2 (PGI2) synthesis in vascular endothelium. TXA2 promotes platelet aggregation by up-regulating integrin surface receptors that cross-link other platelets with fibrinogen to stabilize a platelet plug, while PGI2 inhibits aggregation by disrupting arachidonic acid induced adhesion. TXA2 can only be replenished by new platelets that develop after about 10 days. However, PGI2 can be renewed much sooner by vascular endothelium. Therefore, the overall balance of activity is shifted against platelet aggregation. A low dose of aspirin is efficacious due to the irreversibility of COX enzyme inhibition and an accumulation effect over a few days. Some 50% of TXA2 is suppressed with a first dose of aspirin. A second dose increases suppression to 90% and full suppression can be maintained by a regular low dose.1 , 2
The beneficial use of aspirin as an anti-platelet therapy is widely accepted in secondary prevention of CV events.3 However, the anti-platelet effect also increases the risk of bleeding. For patients who have not yet experienced a CV event, the benefits of the anti-platelet effect in primary prevention of CV events do not outweigh the bleeding risks associated with aspirin.
'Hippocrates offered pregnant women willow leaves in order to ease labour pains'
Studies on effectiveness of aspirin use in primary prevention
Multiple published studies consistently show that the use of low dose aspirin for primary prevention of CV events does not provide net benefit to patients. Perhaps the most comprehensive of these studies in recent years was the Antithrombotic Trialists’ Collaboration in 2009.4 Researchers assessed trials of aspirin use in 95,000 individuals in primary prevention and 17,000 individuals in secondary prevention. They undertook collaborative meta-analyses of serious vascular events (i.e., MI, stroke, vascular death) as well as major bleeds. They found that aspirin allocation for primary prevention yielded a 12% reduction in serious vascular events (mainly due to a reduction of just under a fifth of non-fatal MI) though had no significant net effect on stroke and no significant difference in vascular mortality was found. However, they found that aspirin use increased major gastrointestinal and extra-cranial bleeds by just over 40%. The study strongly supports the view that aspirin does not achieve net benefit in primary prevention as the reduction in CV events is offset by an increase in major bleeds.
The point is further underlined by researchers at the Drugs and Therapeutics Bulletin. They reviewed several meta-analyses in 2009 and found that the benefits of MI or stroke prevention do not outweigh the increased risk of gastrointestinal bleeding.5 They proposed that the use of low dose aspirin for primary prevention of MI and stroke in patients with no CVD had no effect on mortality and should not be routinely initiated, even in those with elevated blood pressure or diabetes. Furthermore, they suggested that people currently on aspirin for primary prevention should review with their doctor whether to continue taking the drug.
In fact, findings that highlight how bleeding risks counterbalance benefits of aspirin use in primary prevention have been echoed in compelling results from several other international studies for several decades. For instance, a randomised trial
of prophylactic daily aspirin in 5,139 British male doctors with no known CVD between 1978 and 1984 found no clear indication of a decrease in mortality from CV events.6 A similar, contemporaneous US study found no reduction in mortality from all CV causes in 22,071 healthy men treated with aspirin or placebo in a randomized trial. The study identified that aspirin helped reduce the risk of MI by 44% but that moderate-severe and fatal haemorrhagic stroke risk was more than doubled.7
More recent studies such as the ‘Hypertension Optimal Treatment’ (HOT) trial further strengthen the argument against the use of aspirin for primary prevention. Aspirin use had no significant effect on cerebral vascular accidents or CV mortality in trials conducted with 18,790 patients for primary prevention across 26 countries. 8 While the HOT study recorded a reduction in MI, it also recorded an increase in major non-fatal bleeds and minor bleeds. Furthermore, a 2005 Women’s Health Study with a randomized trial of 39,876 healthy women treated with aspirin or placebo failed to show any significant improvement in the primary prevention of non-fatal MI, stroke or death from CVD.9
Some guidelines recommend the use of low dose aspirin in patients with type 1 or 2 diabetes for primary prevention of CV events. However, the Prevention of Progression of Arterial Disease and Diabetes (POPADAD) and the Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JPAD) trials both concluded in 2008 that there is no evidence to support the use of aspirin in primary prevention in patients with type 1 or 2 diabetes. In fact, POPADAD found that deaths from coronary heart disease or stroke among were higher among aspirin users compared to non-aspirin users (6.7% v 5.5%).10,11
A random sampling study of 88,698 aspirin users in Taiwan published in 2015 showed that the bleeding risk of regularly taken low dose aspirin cancelled any contribution to preventing major vascular disease. Patients who used low dose aspirin occasionally (less than 20% of the time) had better health outcomes than those who used it regularly (more than 80% of the time).12
A BMJ editorial on the use of aspirin in prevention of cardiovascular events reported that studies have consistently failed to demonstrate net benefits for primary prevention in patients without CVD.13 It cited a review by the US Food and Drug Administration (FDA) of the proposed labelling of aspirin for primary prevention, which evaluated five primary prevention trials, none of which showed net benefits from aspirin use in primary prevention.14 These trials also failed to show a benefit in patients with diabetes or a Framingham risk score greater than 8-10% over 10 years.
All of the literature reviewed points to a consistent conclusion: any benefits of aspirin use for primary prevention of CV events are counterbalanced by potentially fatal bleeding risks.
RELEVANT GUIDELINES
There are several UK and European guidelines that describe aspirin use in patients for primary prevention of CVD. However, it should be noted that these guidelines were published between 2005 and 2008, prior to the most recent research, which highlights the risks of aspirin in primary prevention.
Three key guidelines are as follows:
The Joint British Societies issued guidance in 2005, recommending aspirin 75mg daily for people over 50 years with a total CVD 10 year risk above 20%, as well as for people with diabetes aged over 50 (or younger if they have had diabetes for more than 10 years or have been receiving treatment for hypertension), once blood pressure has been controlled to 150/90 mmHg or less.15
- The Fourth Joint Task Force of the European Society of Cardiology (ESC) guidelines recommended in 2007 that patients take aspirin 75mg daily if their 10-year risk of CVD mortality is over 10% and blood pressure is less than 140/90mmHg.1 6
- The National Institute for Health and Clinical Excellence (NICE) published a guideline in 2008, recommending aspirin 75mg daily for people over 50 years with type 2 diabetes if their blood pressure is below 145/90mmHg.17
In the light of the most recent research (specifically the Drugs and Therapeutics Bulletin research described above), the Irish College of General Practitioners confirmed that aspirin should only be taken on the advice of a GP or healthcare professional. The National Medicines Information Centre at St. James’s Hospital, Dublin, outlined that aspirin mono-therapy is no longer recommended for certain primary prevention such as atrial fibrillation related thromboembolic events, due to the risk of bleeding as well as the observation that the anti-thrombotic effect of aspirin appears to lessen with age.18 The ESC also updated its guidelines based on recent research to state that aspirin is not recommended in individuals with cardiovascular or cerebrovascular disease due to the increased risk of major bleeding. It appears that the guidelines are slowly changing to reflect the evidence on risks of aspirin use in primary prevention.19
SAMPLE EVIDENCE OF COMMON USE OF ASPIRIN FOR PRIMARY PREVENTION
An audit was conducted at the Dun Laoghaire Surgery, Co. Dublin, as part of this review to identify patients who were taking aspirin for primary prevention that did not meet any of the above guidelines.
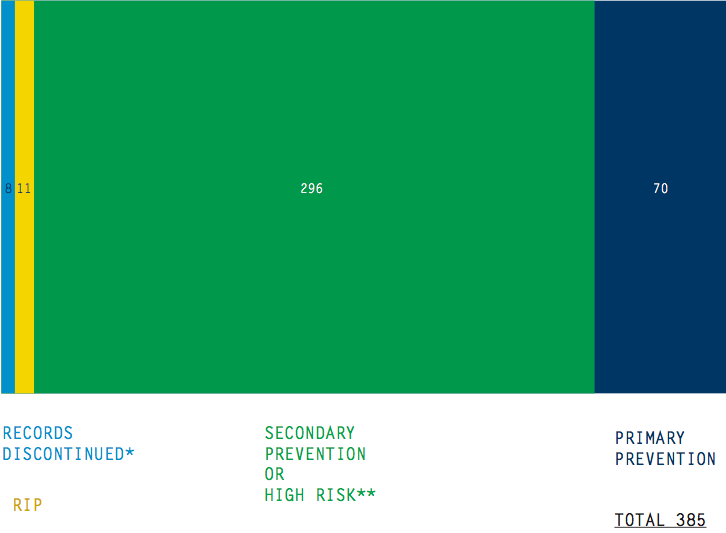
All patients at the practice that had been taking aspirin (75mg daily) in the 24 months prior to July 1, 2013, were identified by a medications search of electronic records. This amounted to 385 patients. 19 of these had either passed away or left the practice in the interim. The histories of each of the remaining 366 patients were reviewed. All those who had experienced a MI, CVA or TIA and therefore were being managed for secondary prevention were excluded. Furthermore, patients with a high CVD or high CV event risk – for instance, those diagnosed with peripheral vascular disease, had demonstrable CV symptoms such as unstable angina or intermittent claudication or who had stents or prosthetic valves in place – were also excluded.
70 patients that had not experienced a CV event and did not fall into the CVD high risk category described above were taking aspirin for primary prevention. These patients had conditions such as controlled hypertension, ‘once-off’ chest pain or had a family history of CV events. These patients amounted to 19% of all current patients taking aspirin for secondary or primary prevention. The 70 patients ranged in age from 35 to 91 years. The median age was 74.5 years, while the average age was 72.4 years.
An audit conducted in the Broadline Family Practice, Blackpool, Cork, in 2011 and 2012 and published in 2013 found results comparable with the Dun Laoghaire audit. 333 patients were identified to be taking aspirin and 62 patients (18.6%) were taking aspirin for primary prevention. Their average age was 64.9 years. It was further determined that 10 of these 62 (16.1%) were at a low risk of cardiovascular disease by calculating their 10-year QRISK2 score.20
Both of these audits indicate that patients in Ireland are often prescribed low dose aspirin for primary prevention of CV events, despite clear and consistent research results showing no net benefit to patients and the introduction of potentially fatal bleeding risk.
Inappropriate use of aspirin for primary prevention does not appear to be an issue unique to Ireland. A study published in 2015 reviewed aspirin use by 68,808 patients in 119 practices across the US and determined that 11.6% of these patients were using aspirin “inappropriately”. The patients had no CVD and their 10-year CVD risk was low. Their use of aspirin introduced risks of gastrointestinal bleeding and haemorrhagic stroke that outweighed benefits in primary prevention.21
BROADENING PREVENTATIVE MEDICINE FOR CVD MANAGEMENT
Prevention of CVD, and all chronic conditions, is a priority for general practice. However, GPs continually make a trade-off between time consuming pro-active preventative medicine and the immediate demands of reacting to acute health conditions. It is estimated that a typical GP would need 7-8 hours to implement best practice preventative medicine each day, precious time that GPs do not have. It is possible therefore that offering aspirin as a preventative measure for CVD may sometimes be seen as an alternative to a more time-consuming assessment of risk factors and investment in education and counselling. For instance, primary care physicians in the US and Australia discuss alcohol consumption with less than a fifth of patients, smoking with two-thirds, exercise with a third and diet with 15-30% - all key modifiable risk factors for CVD.23,24 Although these interactions may take time, the US Preventative Services Task Force identified such risk factor discussions as among the most valuable preventative services to patients in reducing mortality and overall healthcare costs.25
The November 2014 conference of the Irish National Institute for Preventive Cardiology (NIPC) highlighted how 50% of over 50s are overweight or obese, 30- 50% have elevated blood pressure, 34% have low rates of exercise, 20% smoke and 16% report alcohol problems.v26 Speakers at the NIPC conference also outlined how CVD was the single largest cause of death in Ireland and that more than 50% of reductions in CVD relate to risk factor changes.27 It would appear there is much room for improvement in reducing risk factors for CV events that can make a major difference to the health of patients.
HOW MIGHT WE BROADEN PREVENTATIVE MEDICINE IN IRISH GP PRACTICES TO ADDRESS CVD RISK FACTORS?
Interestingly, financial incentives do not appear to help. Only one out of eight financial incentive programmes implemented between 1966 and 2002 in English speaking countries motivated doctors to provide more preventative care.28
The answer may lie instead in introducing planned health checks for all patients over the age of 45. A randomised controlled trial of 1,507 Danish patients showed that the number of patients at elevated cardiovascular risk was halved as a result of biannual health screenings in family practices over five years. The approach is similar to the ‘Managed Care’ philosophy implemented by Kaiser Healthcare in the US, which offers five annual planned health checks to patients over 65, reducing the incidence of acute care emergencies, decreasing the days spent in a hospital bed and improving overall outcomes.
Health check activities could be shared between practice nurses and doctors to help manage limited time resources. This form of preventative medicine where patients and healthcare professionals actively collaborate on managing smoking, alcohol, diet and exercise would lead to improved health outcomes, lower healthcare costs and help avoid unnecessary prescription of aspirin and consequent bleeding risks in primary prevention.
CONCLUSION
Evidence in the literature points to significant risks of bleeding associated with aspirin use that counterbalance benefits in primary prevention of CV events. Despite this, fact-based audits highlight that use of aspirin for primary prevention of CVD and CV events is common. The fact that UK and European guidelines do not reflect the most recent research on the issue may contribute to this. This paper offers three suggestions to address the issues of aspirin use in primary prevention in
light of the above findings. Firstly, doctors should engage with patients who take aspirin for primary prevention to review the full benefits and risks. Secondly, it is worthwhile for doctors and patients to invest time in identifying and managing modifiable risk factors for CVD and conduct regular, planned health checks. Lastly, relevant guidelines should be updated to reflect recent research on the bleeding risks of using aspirin in the prevention of CVD and CV events. These findings and suggested actions could be communicated effectively through the medium of the National Institute for Preventative Cardiology Alliance, which brings together healthcare providers, institutions and industry in preventive action. Putting these suggestions into practice would improve overall healthcare and patient outcomes.
ACKNOWLEDGEMENTS
Thanks to Dr. Nicola Boyle, Dr. Paul Lacey and Dr. Ray Murphy of the Dun Laoghaire Surgery for in- viting me to participate in their audit and for their mentorship.
References
- Pignone M, Williams C. Aspirin for primary prevention of cardiovascular disease in diabetes mellitus. Nat Rev Endocrinol. 2010; 6(11):619-28.
- Rang H, Dale M, Ritter J, Moore P. Pharmacology. 5th edition. London: Elsevier Churchill Livingstone; 2003.
- Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of anti-platelet therapy for prevention of death, myocardial infarction and stroke in high risk patients. BMJ. 2002; 324(7330):141.
- Antithrombotic Trialists’ Collaboration. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomized trials. Lancet. 2009; 373(9678):1849-60.
- Aspirin for primary prevention of cardiovascular disease? Drug Ther Bull. 2009; 47:122-5.
- Peto R, Gray R, Collins R, Wheatley K, Hennekens C, Jamrozik K, Warlow C, Hafner B, Thompson E, Norton S, Gilliland J, Doll R. Randomised trial of prophylactic daily aspirin in British male doc- tors. BMJ. 1988; 296 (6618):313-16.
- Final report on the aspirin component of the ongoing Physicians’ Health Study. Steering committee of the Physicians’ Health Study research group. N Eng J Med. 1989; 321(3):129-35.
- Hansson L, Zanchetti A, Carruthers G, Dahlof B, Elmfeldt D, Julius S, Menard J, Heinz Rahn K, Wedel H, Westerling S. Effects of intensive blood pressure lowering and low dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomized trial. Lancet. 1998; 351(9118):1755-62.
- Ridker P, Cook N, Lee I, Gorden D, Gaziano J, Manzon J, Hennekens C, Buring J. A randomized trial of low dose aspirin in the primary prevention of cardiovascular disease in women. N Eng J Med. 2005; 352(13):1293-304.
- Belch J, MacCuish A, Campbell I, Cobbe S, Taylor R, Prescott R, Lee R, Bancroft J, MacEwan S, Shepherd J, Macfarlane P, Morris A, Jung, R, Kelly C, Connacher A, Peden N, Jamieson A, Matthews D, Leese G, McKnight J, O’Brien I, Semple C, Petrie J, Gordon D, Pringle S, MacWalter R. The prevention of progression of arterial disease and diabetes (POPADAD) trial: factorial randomised placebo controlled trial of aspirin and anti-oxidants in patients with diabetes and asymptomatic peripheral arterial disease. BMJ. 2008; 337:a1840.
- Ogawa H, Nakayama M, Morimoto T, Uemura S, Kanauchi M, Doi N, Jin- nouchi H, Sugiyama S, Saito Y, Japanese primary prevention of atherosclerosis with aspirin for diabetes (JPAD) trial investigators. Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: a randomized controlled trial. JAMA. 2008; 300:2134-41.
- Wu I, Hsieh H, Wu M. A short-term risk–benefit analysis of occasional and regular use of low-dose aspirin in primary prevention of vascular diseases: a nationwide population-based study. BMJ Open [Internet]. 2015 Jan;5:e006694. Available from: http://bmjopen. bmj.com/content/5/1/e006694.full
- Editor. Aspirin for prevention of cardiovascular events. BMJ. 2008; 337:a1806.
- Fleming T, Nissan S, Borer J, Armstrong P. Report from the 100th cardiovascular and renal drugs advisory committee: US Food and Drugs Administration. Circulation. 2004; 109:e9004-5.
- JBS 2: British Cardiac Society, British Hypertension Society, Diabetes UK, Heart UK, Primary care cardiovascular society, The Stroke Association. Joint British Societies’ guidelines on prevention of cardiovascular disease in clinical practice. Heart. 2005; 91:v1-52.
- Fourth Joint Taskforce of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice. European guidelines on cardiovascular disease prevention in clinical practice. Eur J Cardiovasc Prev Rehab. 2007; 14(suppl2):S1-113.
- The National Collaborating Centre for Chronic Conditions. Type 2 diabetes: National clinical guideline for management in primary and secondary care (update). London: NICE, 2008.
- National Medicines Information Centre. Update on management of non-valvular atrial fibrillation, volume 19, number 1. Dublin: St. James’s Hospital, 2013.
- Perk J, De Backer G, Gohlke H, Graham I, Reiner Z, Verschuren M, Albus S, Benlian P, Boysen G, Cifkova R, Deaton C, Ebrahim S, Fisher M, Germano G, Hobbs R, Hoes A, Karadeniz S, Mezzani A, Prescott E, Ryden L, Scherer M, Syvanne M, Scholte op Reimer W, Vrints C, Wood D, Zamorano J, Zan- nad F. European guidelines on cardiovascular disease prevention in clinical practice. The fifth joint taskforce of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice. Eur Heart J. 2012; 33:1635-1701.
- 20 Hallihan P, Horgan T, English T. Who should and shouldn’t be on aspirin? ICGP Forum. 2013; Nov:44-45.
- 21 Hira R, Kennedy K, Nambi V, Jneid H, Alam M, Basra S, Ho M, Deswal A, Ballantyne C, Petersen L, Vira- ni S. Frequency and practice-level variation in inappropriate aspirin use for the primary prevention of cardiovascular disease. J Am Coll Cardiol. 2015; 65(2):111-121.
- 22 Russell G. Is prevention unbalancing general practice? Med J Aust. 2005; 183(2):104-105.
- 23 Stange K, Flocke S, Goodwin M, Kelly R, Zyzanski S. Direct observation of rates of preventive service delivery by community family practice. Prev Med. 2000; 31:167-76.
- National Preventative Health Taskforce. The role of primary health care in preventing the onset of chronic disease, with a particular focus on the lifestyle risk factors of obesity, tobacco and alcohol. Sydney: UNSW Centre for Primary Health Care and Equity, 2008.
- Maciosek M, Coffield A, Edwards N, Flottemesch T, Goodman M, Solberg L. Priorities among effective clinical preventive services: results of a systematic review and analysis. Am J Prev Med. 2006; 31(1):52-61.
- Smyth B. The challenges for prevention in Ireland. In: Pushing the boundaries in cardiovascular disease prevention; 2014 November 29; Galway, Ireland. Dublin: NIPC; 2014.
- Graham I. Enhancing CVD prevention in Ireland. In: Pushing the boundaries in cardiovascular disease prevention conference; 2014 November 29; Galway, Ireland. Dublin: NIPC; 2014.
- Town R, Kane R, Johnson P, Butler M. Economic incentives and physicians’ delivery of preventive care: a systematic review. Am J Prev Med. 2005; 28:234-240.
- Engberg M, Christensen B, Karls- mose B, Lous J, Lauritzen T. General health screenings to improve cardiovascular risk profiles:a randomized controlled trial in general practice with 5-year follow-up. J Fam Pract. 2002; 51(6):546-52.